

The Mifepristone Maze
How courts turned one FDA-approved medication into a national test of rights, access, and confusion

📌 NOTE FOR NEW READERS: This is an independent publication covering 50501, No Kings, and the broader pro-democracy and civic-action ecosystem. Subscribe to join our community and to keep us posting.
Between Friday and Monday, Mifepristone medication went from legally restricted to temporarily restored.
Mifepristone has been FDA-approved since 2000. A generic has been available since 2019.
It’s been part of the standard of care for a quarter century. And at this moment in time, whether a patient can access it depends less on medical evidence than on which court ruled most recently.
On Friday, a federal appeals court blocked mifepristone from being mailed or dispensed at pharmacies and by Monday, the Supreme Court had paused that order.
Providers froze prescriptions over the weekend, patients canceled appointments, some pharmacies pulled the drug from shelves and then put it back.
This is Mifepristone whiplash. We’re walking through the maze so we can see where the walls are, and how to get out.
The Civic Clarity Maze
At each step in the maze, when we hit a wall, we ask a question: Is this clarity, distraction, or a pressure point?
Clarity means we know what happened and can explain it.
Distraction means people are being forced to make consequential decisions under manufactured uncertainty.
A pressure point means there’s still somewhere public attention, civic pressure, or organized response can change the outcome.
The point of this is to help make it understandable. When a legal fight becomes too complicated to follow, confusion narrows access. Making the issue easier to understand, explain, and to act on.
Wall One: What Even Is Mifepristone?
Mifepristone is one of two medications used in the standard medication abortion regimen. The FDA’s own labeling states that mifepristone is used with misoprostol to end an intrauterine pregnancy through 10 weeks gestation.
But the clinical reality extends further than that framing suggests. The American College of Obstetricians and Gynecologists has been clear that mifepristone is used for both abortion care and miscarriage management. The political fight over this medication doesn’t stay in just one category. Legal restrictions on mifepristone move through the broader systems patients and clinicians rely on for time-sensitive reproductive care, including care that has nothing to do with elective abortion.
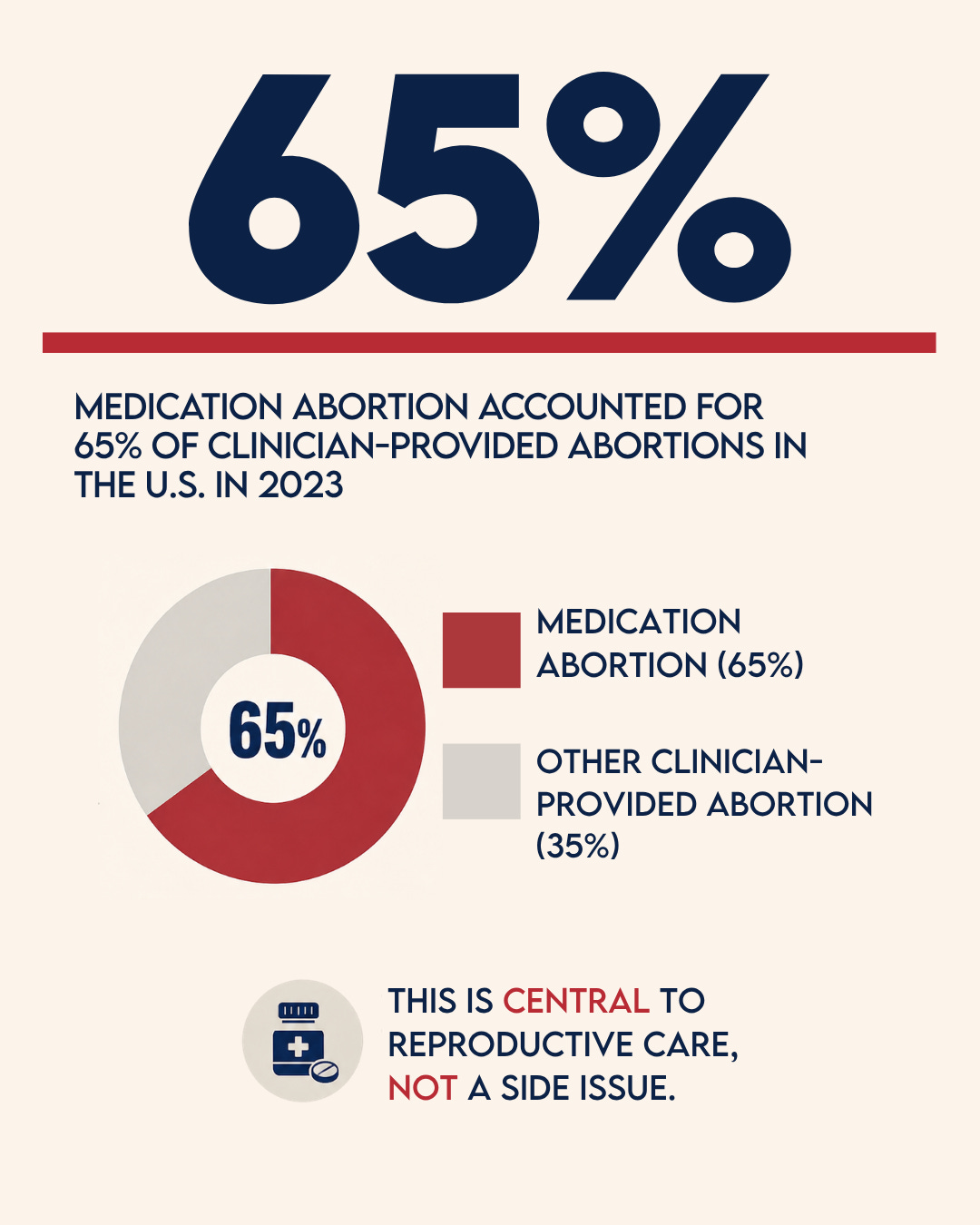
Medication abortion is also not a fringe practice.
The Guttmacher Institute reports that medication abortion accounted for 65% of all clinician-provided abortions in the United States in 2023, up from 53% in 2020. This legal fight affects the central pillar of reproductive health care delivery in this country, not an edge case.
Maze check: Clarity.
We know what the medication is.
We know it has been FDA-approved for decades.
We know medication abortion is now the majority method of clinician-provided abortion care in the United States.
The clinical evidence supporting mifepristone’s safety and efficacy hasn’t changed.
What’s in dispute is if courts can override the FDA’s regulatory conclusions about how that medication should be dispensed.
Wall Two: What Changed?
On May 1, the U.S. Court of Appeals for the Fifth Circuit issued a ruling that restricted access to mifepristone by blocking mail distribution and reinstating an in-person dispensing requirement.
It reverses the FDA’s 2021 decision to remove the in-person dispensing requirement, a decision the agency formalized in 2023 after concluding that expanded telehealth and mail distribution were safe and appropriate.
The FDA, KFF, and the ACLU all point to years of safety data and real-world use supporting the current dispensing rules, but the Fifth Circuit credited Louisiana’s argument that the FDA had not adequately justified allowing remote dispensing without additional safeguards. The case came from Louisiana’s challenge to the FDA’s regulatory authority.
Under the Federal Food, Drug, and Cosmetic Act, Congress gave the FDA authority to regulate drugs nationwide, including how they are prescribed and dispensed.
That authority exists so drug safety standards are determined by scientific evidence evaluated at the federal level, not by individual state litigation strategies.
Maze check: Distraction.
When a court ruling can abruptly reverse how a medication is accessed nationwide, patients are not dealing with law in any functional sense. They’re dealing with uncertainty at the exact moment when clarity matters most. A patient seeking time-sensitive care can’t wait for the appellate calendar.
Wall Three: What Did the Supreme Court Do?
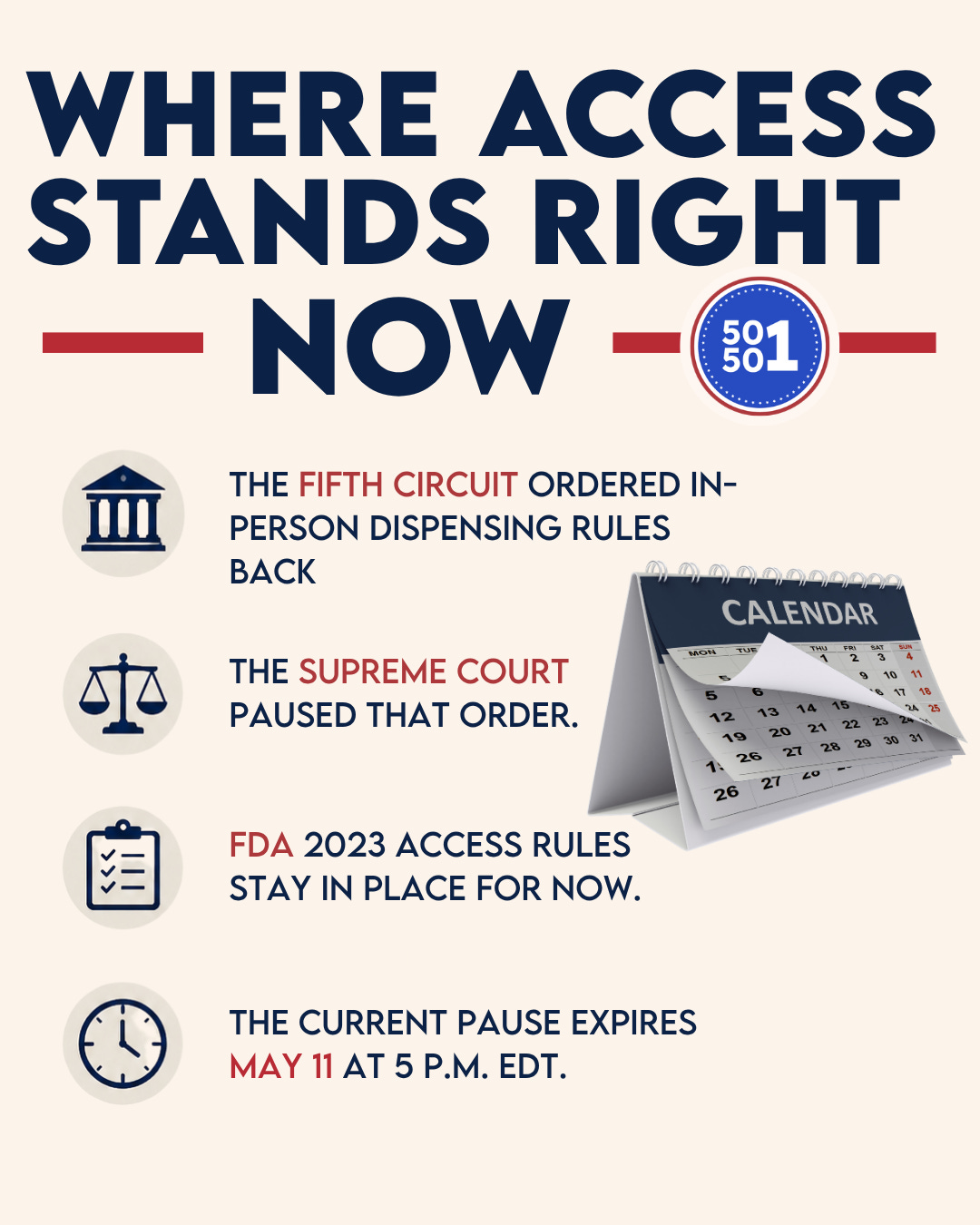
On May 4, the Supreme Court administratively stayed the Fifth Circuit’s order, temporarily blocking it from taking effect while the Court considers emergency appeals from mifepristone manufacturers. AP reported that Justice Samuel Alito’s order allows telehealth, mail, and pharmacy access to continue under the FDA’s 2023 rules while the Court considers what to do next.
The ACLU described the order as a one-week pause, lasting until May 11, while the Court considers whether to block the Fifth Circuit’s ruling for a longer period.
This was a temporary administrative hold. The Supreme Court did not say the Fifth Circuit was wrong. The Court said, in effect, that the status quo should be preserved while the justices decide how to proceed.
For now, the immediate federal restriction is paused. But the legal fight underneath it remains active, the stay expires at 5 p.m. EDT on May 11, and access continues to depend on state law, local provider availability, and pharmacy policy.
Maze check: temporary clarity.
The pause expires on May 11.
Wall Four: Why Does This Feel So Disorienting?
Because the effect is disorienting, whether or not confusion is the stated goal of any party to this litigation.
Axios reported that the legal back-and-forth has caused confusion for pharmacies, telehealth providers, clinicians, and patients, including in states where abortion remains fully legal.
Some providers reportedly paused teleprescribing entirely while they waited for the courts to act.
In states where abortion is legal, where no state restriction applies, providers still hesitated because the federal legal landscape had become too unstable to interpret confidently in real time.
Rights can become functionally inaccessible when people don’t know what’s legal, when providers hesitate out of legal caution, when pharmacies wait for compliance guidance, when state and federal rules appear to collide, and when patients are left trying to interpret emergency court orders instead of focusing on their own medical decisions.
Confusion is one of the primary ways access gets narrowed. Clear information, under these conditions is a civic resource.
Maze check: Distraction plus pressure point.
The Distraction is the not-knowing. The pressure point is public clarity.
Access by Confusion

Since the Supreme Court overturned Roe v. Wade in Dobbs, abortion access has not been governed by one national standard. It has been shaped by a shifting patchwork of state bans, court injunctions, provider decisions, pharmacy policies, federal agency rules, emergency motions, and temporary pauses.
And keep in mind that the patchwork doesn’t affect everyone equally.
People with financial resources, flexible schedules, reliable transportation, internet access, and supportive personal networks can often find a path through the maze. People without those advantages face the hardest version of it.
The single parent working hourly shifts who can’t take a day off to drive to another state. The patient in a rural area without broadband who can’t access telehealth. The young person without a credit card or a car.
Choose Your Civic Role
The Explainer
Choose this if people in your life ask you when they are confused.
Your mission: explain what happened in easy to understand terms.
The facts: A federal appeals court temporarily ordered the FDA to reinstate in-person dispensing rules for mifepristone. The Supreme Court administratively stayed that order until May 11 while it considers emergency appeals. For now, the FDA’s 2023 access rules remain in place, meaning telehealth, mail, and certified pharmacy dispensing can continue where otherwise allowed. Access still depends on state law, provider availability, pharmacy policy, and what the Court does next.
That’s enough. Not every conversation needs a law-review article. Sometimes democratic resilience starts with one person saying, calmly and accurately, “Here is what actually happened.”
The Sharer
Choose this if you do not have energy for a phone call today but can help stop confusion from spreading.
Your mission: share a verified source with someone asking, “Wait, what is actually going on?” Send this article or share the FDA’s mifepristone information page, the ACLU’s case update, or AP’s Supreme Court coverage.
The goal is not to worry anyone to the point of panic. Replace confusion with something reliable.
The Caller
Choose this if you have 10 minutes and want to apply direct civic pressure.
Your mission: call or email one elected official and ask where they stand on protecting access to reproductive health care, medication abortion, miscarriage care, and FDA regulatory authority.
*We provided you with a script below if you don’t know what to say.
The Local Guide
Choose this if you like helping people find information.
Your mission: drop a comment with your state and a reliable state-level reproductive health resource. This turns the comment section into a practical, crowd-sourced reference readers can use across the country. Your resource might be what someone is actively looking for.
The Rested Resister
Choose this if you are exhausted.
Your mission: save this article and come back when you are ready.
Civic engagement can’t survive if you burn yourself out responding to every emergency. Staying engaged might mean choosing the smallest possible step and refusing to quit. Rest up, you’ve got this.

The 10-Minute Action Guide
If you have 10 minutes today, choose the path of your civic role, or try something new.
Path One: Save the guide. Keep this post as a reference if the legal landscape shifts again.
Path Two: Share the guide. Forward this to someone who is confused, overwhelmed, or trying to understand what changed.
Path Three: Make a call. Contact an elected official and ask where they stand on protecting access to medication abortion, miscarriage care, and FDA-approved medication.
Path Four: Help another reader. Leave a comment with your state and a medical resource.
Call or Email Script
Hello, my name is *NAME, and I am a concerned constituent.
I am calling to ask *OFFICIAL NAME to support access to reproductive health care, including medication abortion and miscarriage care.
The recent court fight over mifepristone has created confusion for patients, providers, pharmacies, and families across the country. People should not have to navigate legal whiplash to access time-sensitive medical care.
Please support policies that protect access to FDA-approved medication, defend the ability of patients and providers to rely on evidence-based regulatory decisions, and prevent courts from creating nationwide disruption before cases are fully resolved.
Thank you.
Clarity Check
This is an obvious attack on women’s rights and reproductive freedom.
This case shows how the attack works: Rights don’t usually just disappear in one move. They are often weakened through what we are experiencing now. Through confusion, delay, provider hesitation, and pharmacy uncertainty.
Right now, Mifepristone is showing us just how unstable and fragile women’s rights are here, in the United States.
What Comes Next
The Supreme Court’s current pause is temporary.
Justice Alito’s administrative stay lasts until 5 p.m. EDT on May 11, with responses due by Thursday, May 7.
After that, the Court will decide whether to block the Fifth Circuit’s order for a longer period while the case proceeds.
This story may change again within days.
When it does, the pressure point may move fast: to Congress, state legislators, FDA authority, legal organizations, providers, pharmacies, voter mobilization, public education, or practical support networks helping patients navigate access.
This is why we can’t afford to get lost in the maze.
Public clarity will help determine how quickly people understand what changed, who is affected, and how we mobilize.
Sources
FDA: Information about mifepristone for medical termination of pregnancy through ten weeks gestation | Questions and answers on mifepristone
ACOG: What to know about abortion and miscarriages with or without mifepristone
ACOG: Medication abortion up to 70 days of gestation
Guttmacher Institute: Abortion in the United States
AP: Court restricts abortion access across the U.S. by blocking the mailing of mifepristone
Supreme Court docket: Danco Laboratories, LLC v. Louisiana, et al.
ACLU: State of Louisiana v. U.S. Food and Drug Administration
Axios: Abortion pill rulings cause whiplash and confusion
KFF: Louisiana v. FDA: Access to Mifepristone Back at the Supreme Court
A woman's right to choose what happens to her body is critical to her freedom. America is becoming less free by the day.
The domination of male over female is never ending. Pardon me for using gender identity in this discussion but it cannot be avoided. Issues of importance often become clouded with debate about terminology. This one is no different. Women have been held to be subservient to men forever. One's value as a human should never be based on gender, race, religion, or any arbitrary measures of worthines. Humanity survives on protecting each of us from oppression. Losing sight of this ideal diminishes our capacity to maintain civilized society. Ignore the obvious at your own peril.